A Vanderbilt University Medical Center study published recently in Child Welfare of “plans of safe care (POSC)” for infants affected by maternal substance use found that there is variability in practice driven by vague policy, challenges of cross-system collaboration and a lack of general knowledge about substance use disorder.
“The opioid crisis has had a substantial effect on pregnant women and infants,” said Stephen Patrick, MD, MPH, professor of Pediatrics and Health Policy, director of the Center for Child Health Policy at VUMC, and senior author of the study, “Opportunities for Child Welfare to Respond to Prenatal Alcohol and Other Substance Exposures.”
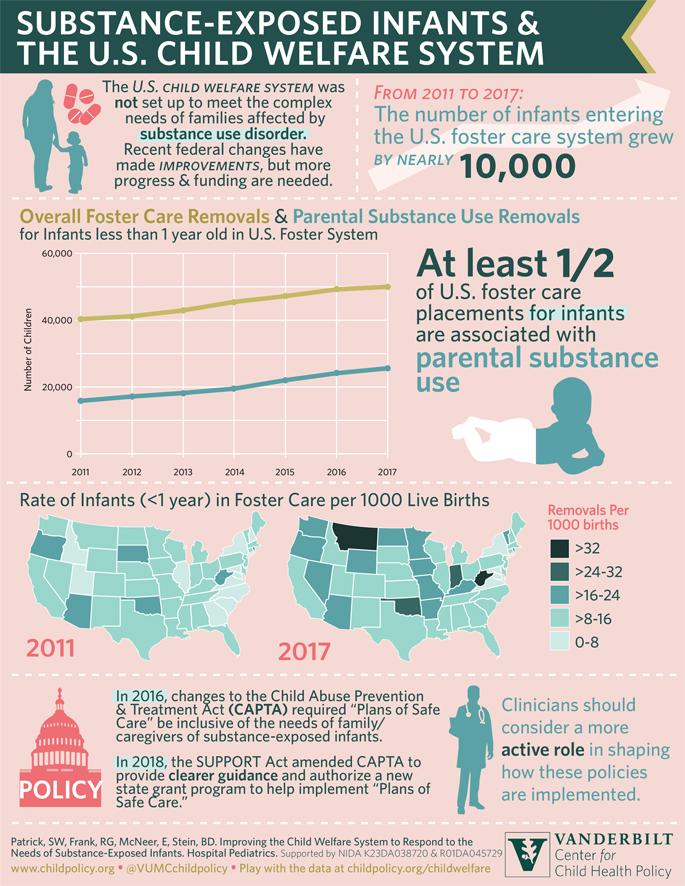
“We’ve seen pretty stark increases in opioid use disorder among pregnant women and record rises in overdose deaths among pregnant women, but one of the crises of the opioid crisis that gets less attention is foster placements. As we’ve seen the rise in overdoses among pregnant women, infants have also become the fastest growing group in foster care in the U.S. today. Most of that is due to parental substance use. These things are linked — the rise in the opioid crisis and the effect it’s having in pregnancy are very much linked to the rapid rise in foster placement,” said Patrick, holder of the Dr. William R. Long Directorship in Children’s Health Policy.
In response, recent federal policy changes added the use of POSC for all substance-affected infants to address the health and substance use disorder treatment needs of the family and ensure the safety and well-being of the infant upon release from health care providers after delivery. Despite taking effect in 2016, little is known about the effectiveness of the policy or how child welfare agencies are implementing the practice locally. This study was a first look into characterizing local barriers and facilitators to POSC implementation.
These effects of POSC implementation are felt locally too at VUMC. The Center for Child Health Policy runs a program called Firefly, a patient-centered service delivery program which aims to improve the quality of care for pregnant and postpartum Medicaid beneficiaries with opioid use disorder and their infants in Middle Tennessee.
“There’s not a week that goes by that we aren’t helping families navigate the child welfare system. While it may seem really separate from the medical care, child welfare and the child welfare involvement are one of the reasons that people avoid care altogether,” Patrick said.
For the study, investigators spoke with county child welfare administrators and managers in nine counties across the U.S.
“The main takeaway is that current policy lacks the detail and accountability for all parties involved in caring for the family to facilitate meaningful POSC implementation,” said Sarah Loch, MPH, director of Research Operations for the Center for Child Health Policy and first author of the study.
“Up until this point it’s really been on the child welfare system alone to implement POSC, but what we heard from the managers and administrators is that they need to collaborate with the medical system because those folks are providing obstetric care and substance use disorder treatment in the community. They’d love to be collaborating with the judicial system because judges are the ones who decide what the custody plan should be for children. Current policy doesn’t ensure buy-in across those sectors or the resources to do so. It’s been left up to child welfare to facilitate collaboration which has made collective work challenging,” Loch said.
Loch also said that one of the limitations of POSC is that child welfare is limited as to when they can start serving the baby and the family.
“In many states they can’t intervene until the child is born. A medical provider might identify a substance use disorder during pregnancy and connect them to child welfare to get a POSC in place, but child welfare can’t actually do that until the baby is born. So, there’s a window of missed opportunity and lack of prevention focus that the policy just doesn’t support right now.”
Patrick said the next step is expanding the work of the pilot study and broadening the scope ― talking more to some of the key players: OB providers, substance use disorder providers and judges in the community. Their group, in partnership with Vanderbilt University, the RAND Corporation, University of Central Florida, University of Connecticut, and Casey Family Programs, was recently awarded a $2.6 million grant from the National Institute on Drug Abuse that will expand this work nationally and will enable quantitative and qualitative analyses.
“We know the perspective of child welfare administrators, but there are so many other players that need to come to the table. We need to understand from their perspectives as well what’s the best way we can be supporting these families.”