Nearly one-fourth of patients who undergo surgery to remove cancer will end up having to go back to their doctor or will require an additional surgery at some point in the not-so-distant future.
One underlying problem is that surgeons can’t see cancer.

“You can’t see it and this has plagued cancer surgeons for a long time because, even though surgery is the curative treatment for most solid tumor types, positive margin rates have not changed in 30 years as the result of poor cancer visualization in the operating room,” said head and neck cancer surgeon Eben Rosenthal, MD, Odess Professor of Otolaryngology – Head and Neck Surgery and chair of the department at Vanderbilt University Medical Center.
Rosenthal has been working to solve the problem for over 15 years and holds multiple investigational new drug (IND) applications being studied in clinical trials at Vanderbilt and his prior institution, Stanford University School of Medicine. The drugs provide a targeted fluorescent dye that clings to and illuminates cancer.
“This technology would add an additional level of precision in resecting these tumors during cancer surgery which is currently not available in real time to surgeons,” said Kamran Idrees, MD, chief of the Division of Surgical Oncology and Endocrine Surgery.
“Complete removal of tumors will not only be beneficial for patients to avoid additional treatments such as radiation therapy and operations but also result in the cost savings for health care systems.”
Trials will be opening soon at both Vanderbilt and Stanford, which has a dedicated facility to make the drugs.
“We have been using it to image cancer that cannot be seen or felt by the surgeon, including lymph nodes. The studies intend to show that this technique will improve the ability to obtain clear margins at the time of surgery,” he said, “and hopefully improve our patient’s quality of life.
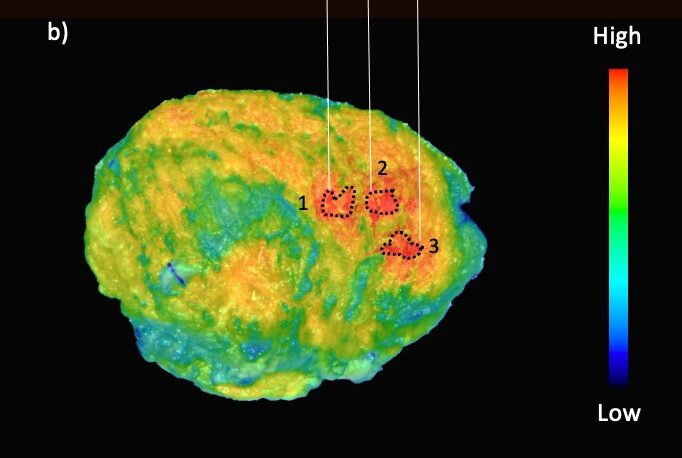
“Our initial results show that it is very effective at seeing the cancer that might be left behind. It has been successful at seeing brain cancer and identifying lymph nodes in head and neck cancer. Applications of these new techniques allow many different opportunities to improve cancer surgery for these patients.”
The drugs, which were in pre-clinical work until 2013 and now clinical work over the last seven to 10 years, work on most solid tumors including colon cancer, pancreatic cancer, head and neck cancer, skin cancer, brain cancer and lung cancer.
The agent has been proven safe in more than 100 patients and works by making the cancer glow during surgery. It is manufactured by modifying a commercially available therapeutic agent and labeling it with a fluorescent probe. When injected, the antibody binds to the cancer and then fluoresces, causing it to glow so surgeons can see it.
“We know that if we can find the margins more effectively we are likely to improve patient outcomes,” Rosenthal said. “There are currently many of these agents in clinical trials, and I think in five to 10 years this will be standard of care for cancer surgery — I want to make sure Vanderbilt is on the cutting the edge of this science.
“Normally, it all just looks like a bunch of hamburger, but when the cancer fluorescence is present the surgeon can know right away if there might be tumor left behind, but without it the surgeon does not know where to test or where to look.”
Rosenthal said the fluorescent dye provides opportunities for finding lymph nodes and secondary lesions that wouldn’t normally be seen.
Over the next six months he will be submitting the IND to the FDA and, hopefully, start infusing patients at VUMC and Stanford.
“We do know for certain that positive margins correlate with a negative outcome, with poor survival,” he said. “This is such a huge problem.”